Quick Takeaway: The next wave of cardiovascular innovation isn’t just in devices; it’s in how procedures are planned. Patient-specific 3D data transforms decision-making, enables more precise device deployment, and expands access to treatment across structural heart (TMTT, TMVR,TAVI,LAA) and vascular (EVAR, PE, DVT) procedures.
From Devices to Data-Driven Decisions
For decades, cardiovascular innovation was defined by the hardware: a more durable valve, a more flexible stent, or a smarter graft. Today, devices alone no longer determine clinical or commercial success.
Outcomes now increasingly depend on how precisely clinicians can interpret patient anatomy, test device fit, and map out each procedure in advance. Even the most advanced device can perform inconsistently if planning relies on flat 2D imaging, manual interpretation, or incomplete anatomical insight.
What’s transformative isn’t just a better device. It’s turning patient-specific anatomy into actionable, data-driven insight before entering the operating room. This enables teams to:
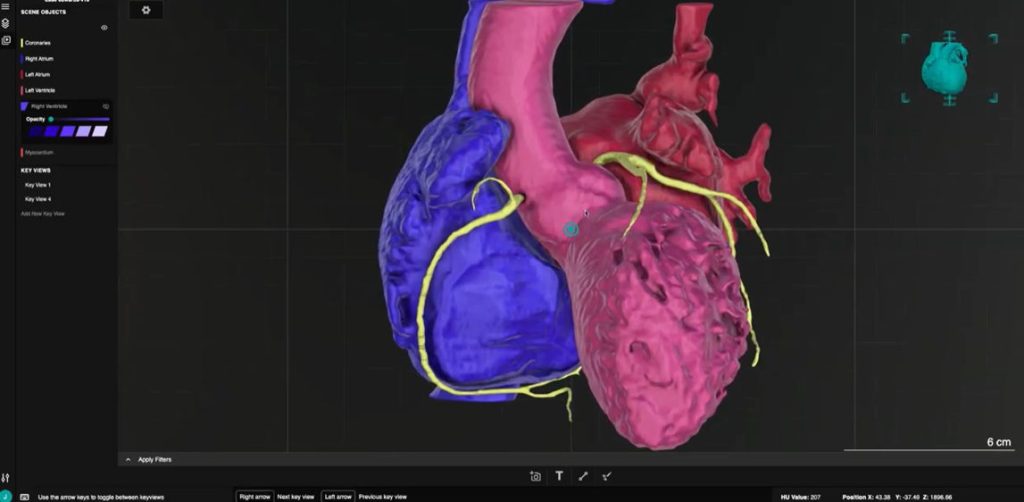
- Fully visualize complex, highly variable anatomy in three dimensions.
- Evaluate device fit, optimal sizing, and deployment strategies dynamically.
- Anticipate procedural challenges to drastically reduce intraoperative uncertainty.
- Standardize planning methodologies across clinicians, centers, and geographies.
Moving Beyond the Screening Bottleneck: Quantifying the “Gray Zone”
The biggest constraint in cardiovascular care today isn’t a lack of device innovation. It’s the screening bottleneck.
Across TMTT, TAVR, and EVAR procedures, an estimated 20% to 30% of borderline patients fall into a clinical “gray zone”. These are patients who are technically viable candidates for treatment, but are ultimately turned away because clinicians are forced to make conservative calls based on ambiguous data.
The Reality of the Status Quo: Traditional 2D imaging and manual interpretation force teams to rely on approximations for critical decisions like landing zones and access strategies. When you are estimating boundaries on a flat screen, the risk profile rises, and patients lose out on life-saving interventions.
By combining 3D anatomical data, automated measurements, and AI-powered planning, teams can eliminate this guesswork. The result is a new standard for patient selection:
- Fewer patients excluded due to measurement uncertainty.
- Greater procedural confidence when navigating complex and borderline anatomies.
- Expanded market access by safely moving patients out of the gray zone and into the OR.
From Approximation to Precision: A Case for Clinical Specificity
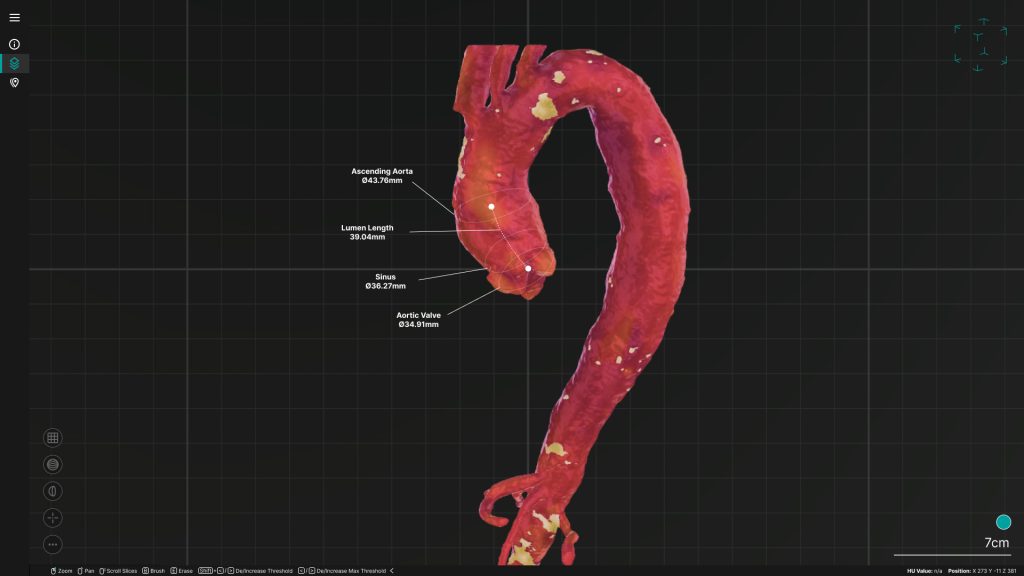
To understand the power of automated 3D data, look at a complex procedure like Transcatheter Mitral Valve Replacement (TMVR).
Traditional 2D CT slices frequently fail to capture the exact, asymmetrical distribution of calcium along the mitral annulus. When a clinical team relies on manual tracking, they are essentially extrapolating how a rigid valve frame will interact with irregular calcification.
Automated 3D modeling removes this blind spot by mapping the entire volumetric density of the calcium. It highlights the exact landing zone and access strategy required, allowing the heart team to foresee and prevent catastrophic complications—such as paravalvular leak (PVL) or device migration, long before the first incision is made.
Addressing the Skeptic: Why Trust the Algorithm?
Naturally, seasoned interventionalists and surgeons meet “automation” with healthy skepticism. Medicine is an art as well as a science, and clinicians rightfully trust their own eyes and decades of experience over a black-box algorithm.
But automated 3D planning isn’t designed to replace clinical judgment; it is designed to eliminate human variability. Manual 2D measurements can vary by as much as 10% to 15% between different observers, or even the same observer on a different day.
For medical device companies, this variability is a significant barrier to technology adoption. When conservative manual math leads clinicians to prematurely turn a patient away, a therapy’s real-world impact is unnecessarily limited.
Conversely, if a device is deployed based on an inaccurate manual calculation and a poor clinical outcome follows, the clinical community often questions the device itself rather than the flawed planning that preceded it.
Automated algorithms process sub-millimeter volumetric data consistently every single time. By providing an undeniable, highly reproducible architectural blueprint, automation doesn’t override the surgeon’s eyes; it protects the integrity of both the procedure and the technology, ensuring the device can perform exactly as it was engineered to.
Breaking Through Internal and Commercial Bottlenecks
The value of automated 3D planning isn’t confined to the operating room. For medtech companies, the current reality of managing patient data is dictated by a complex, fragmented internal workflow. Processes span from R&D and clinical development to clinical trials screening. Too often, these workflows rely on a disconnected patchwork of manual steps, imaging systems, and third-party tools.
This fragmentation creates severe operational friction:
- The Segmentation Bottleneck: Manual segmentation for complex structural heart cases is incredibly time and resource-intensive, dragging down personalized planning and device workflows.
- Turnaround Pressure and Step Fatigue: Protracted planning timelines directly cause delays in procedural scheduling, frustrating interventionalists who face immense pressure to maintain efficient patient flow amid rising case volumes.
- Limited Scalability: As therapy volumes grow, a heavy reliance on manual processes introduces institutional variability and creates an operational ceiling that inhibits commercial scaling.
By consolidating these disparate processes into a single, unified platform, medtech companies can eliminate step fatigue, slash planning timelines, and deliver the rapid, automated turnaround times that modern clinicians demand.
The New Baseline for Cardiovascular Portfolio Growth
The next phase of growth in cardiovascular medtech will extend far beyond iterative hardware engineering. To truly scale advanced therapies, device manufacturers must look to automated, patient-specific planning as a core component of their commercial and clinical strategy. Integrating scalable AI and 3D automation allows medical device companies to:
- Accelerate Therapy Adoption Globally: High-fidelity 3D models can be generated rapidly and at scale across massive patient volumes. This gives lower-volume and regional centers the clinical confidence they need to safely adopt complex procedures and utilize advanced devices.
- Standardize Clinical Support and Reduce Field Burden: By automating how complex anatomy is interpreted across multiple clinical sites, manufacturers can establish a highly reproducible, digital baseline for patient screening. This mitigates reliance on intensive, variable manual support from field clinical specialists.
- De-Risk Portfolio Expansion: Standardizing the procedural planning phase minimizes the institutional and operator variability that can compromise real-world outcomes. This ensures that new, highly technical device portfolios perform predictably and achieve consistent results, no matter the site.
The Verdict
Better data transforms imaging from a limitation into a predictable foundation for portfolio growth. The most successful cardiovascular companies will no longer compete solely on hardware features; they will compete on the speed and precision of the decisions they enable.
In three years, selling a structural heart device without automated 3D procedural planning will be like selling a smartphone without an operating system. The future of medtech innovation belongs to companies that own the data-driven insight before the first incision is ever made.
